
First, I will very briefly summarize the high points of the first two presentations to set the stage for this one. In the first one, I reviewed scientific research that indicated that what we believe about the world and what we occupy our minds with impacts our health. Scientific studies were reviewed that demonstrated that being involved with the New Testament teachings in our lives is healing. In the second presentation, what Jesus declared about the power of the human mind was examined. Research demonstrating the power of the placebo effect and what has been called “spontaneous remission of incurable diseases” confirms his statements.
Embedded within the details of the first two presentations, though, is an important theme that points the way towards a deeper understanding of the nature and causes of human illness and disease. Instead of the causes and risk factors for each disease being specific to that disease, we are finding that trauma and unpleasant experiences increase the likelihood that many different diseases might develop, or causes them to get worse, in a very general fashion. Instead of each disease only responding to medications and other physical interventions specific to that disease, we are finding that being involved with uplifting and positive ideas in our lives tends to prevent or heal all disease, also in a very general fashion.
As we follow this theme further, and as we include more insights from the New Testament Gospels that are supported by extensive scientific research in our exploration, we will expand our understanding of human disease. We will uncover the origins of most mental and physical illness, and we will discover how our misunderstanding of the true nature of chronic diseases has impeded our ability to both prevent them and heal them. Research has also shown that the use of these insights promotes longer and happier lives.
Let us now look at some important New Testament passages pointing towards the true causes of illness.
What are “unclean spirits”?
First, consider what everyone believed about the nature of disease when Jesus was teaching two thousand years ago. Obviously, there was no knowledge of things like microbes, genes, and human anatomy that we take for granted today. Lacking these modern insights, illness was assumed to be the result of the actions of evil spirits, sometimes called Satan or devils. Those with disease were believed to be possessed by these spirits, and if their disease was cured, it was concluded that the spiritual possession was “cast out.” Lacking our modern knowledge, these concepts were natural inferences that were quite compelling.
To fully comprehend what Jesus was teaching about illness and its cure, we should keep in mind that he had to use concepts and language that the people he was addressing could relate to, and he could only reach them through the terminology of their beliefs. Because disease was believed to be the result of evil spirits, it was taught in these terms. To further complicate things, virtually all his teachings involved spiritual concepts that the people of his time had no words to clearly describe, therefore his teachings almost always involved metaphors. Consider also that Jesus did not write anything as he was teaching. Since what we have available to us in the Gospels is only what his disciples remembered of his teachings, their recollections were likely to have been further distorted by their ideas about what caused disease.
To better clarify what I am saying here, I will provide a few passages from the Gospels that illustrate these insights along with commentary that describes our modern understanding of what the Gospel writers were describing.
This first passage, from Matthew 17:14-18, describes a boy who probably had a seizure disorder, and Jesus’ cure was described as the rebuking of the devil that possessed him:
“And when they were come to the multitude, there came to him a certain man, kneeling down to sating, Lord, have mercy on my son; for he is a lunatic, and sore vexed; for oftimes he falleth into the fire, and oft into the water. And I brought him to thy disciples and they could not cure him. Then Jesus answered and said, O faithless and perverse generation, how long shall I be with you? Bring him hither to me. And Jesus rebuked the devil: and he departed from him: and the child was cured in that very hour.”
We now know many of the causes of seizures and how to control or cure them, but none of our treatments involve the casting out of devils. This is not to say that Jesus did not cure this boy as described, only that the ancient description of what happened was, of necessity, distorted and misleading, if taken literally.
Another example is found in Luke 13:11-16, where we are told that Jesus cured a woman of a prolonged infirmity which had her bowed forward so she could not stand upright. This was likely arthritis or osteoporosis, but Jesus was quoted as saying Satan had bound her for eighteen years and that he had then loosed Satan’s binding. In Matthew 12:22, a man blind and unable to speak was brought to Jesus. The man was described as being possessed with a devil, and Jesus cured him also.
In further passages we are told that all of the diseases that Jesus cured were from the same source. In Matthew 8:16, it was reported how a number of people seeking healing were brought to Jesus and they were all described as being possessed by devils. This illustrates clearly that in Jesus’ time, illness was attributed to possession by devils:
“When the even was come, they brought hime many that were possesed by devils; and he cast out the spirits with his word, and he healed all that were sick.”
In Matthew 10:1, the writer of this Gospel also describes the power that Jesus gave to his disciples to heal as being the power to cast out evil spirits.
“And when he called unto him his twelve disciples, he gave them power against unclean spirits, to cast them out, and to heal all manner of sickness and all manner of illness.”
For people in ancient times to conclude that the cause of human illness was due to the action of “unclean spirits” was not completely unreasonable. Since the Gospel teachings were addressing a cause of disease that was invisible, it was natural to assume it was spiritual. It also seemed to be a single, powerful force with evil intent, since it produced so many different deadly diseases, and it appeared to act as if it was possessing the individual and continuously damaging the unfortunate person possessed by it. In the language of this metaphor of being possessed by evil spirits, there might have been ways to free the diseased person from their possession. The result would then seem like the “casting out” of the “unclean spirit.”
Next, I will describe the high points of a newly developing field of research that started with a seminal study of what has been called “adverse childhood experiences” and how they might impact human health and disease later in life. This research is pointing the way towards a deeper understanding of chronic illness that is remarkably similar to the ancient image of being possessed by “unclean spirits.”
The ACE Study story
In the mid 1980’s, Vincent Felitti MD, was helping patients in an obesity treatment program for the Kaiser Permanente HMO in California. He made two important observations of the people he was treating. First, he noted that some of the most successful patients dropped out of the program, rejecting the strategies that had been effective, and regaining the weight they lost. He also noticed how many of his obese adult patients had reported being abused as children, reporting these experiences much more often than his normal weight patients. To explore the implications of his observations, he interviewed 286 of his patients in depth and confirmed his suspicion that overeating was often a partial solution to emotional problems that started with being traumatized as children.
Then, in 1990, he presented a report on these observations at an obesity conference. After his presentation, Robert Anda MD, who had been researching the connection between depression and heart disease, suggested that they collaborate with their research. Dr. Anda proposed a formal study of Kaiser Permanente patients that would broaden the approach to looking at the relationship of childhood trauma to the emergence of emotional and physical health problems later in life.
The research team developed a 10-question survey to measure adverse childhood experiences, calling it the “ACE questionnaire”. They then enrolled 9,508 Kaiser Permanente patients in their research project who had well documented medical histories. This rich source of personal historical information allowed them to easily compare the survey results with each research subject’s medical histories as adults. They found that not only where trauma exposures a lot more common than expected, the relationship with illness later in life was much more powerful than they would have imagined. These findings were ground-breaking. Prior to this study, early-life traumas were not considered as potential causes for adult disease.
But are the dramatic results of this study reliable? Yes. They have been replicated in hundreds of subsequent studies, including surveys in other countries and racial groups. Subsequently, more focused research has not only further confirmed the initial reports, it has also greatly expanded our understanding of the various factors involved. As I proceed in this analysis of some of the root causes of human disease, I will abstract pertinent findings and conclusions from this large body of research to provide a sound introduction to help understand what it is all telling us. As in my previous presentations, some of the most important research studies I am drawing from will be cited in the references at the end.
As a first step in this exploration, I will examine the findings of how childhood traumas become sources of continuous emotional discomfort and distress later in life. This will then give us the foundation for understanding other important health consequences that appear to also result from early-life physical and emotional injury.
Adverse childhood experiences and chronic emotional discomfort
Before looking at the relationships the Adverse Childhood Experience Study found, it may be helpful to consider the categories of distress the ACE questionnaire used. All types of abuse were addressed: physical, emotional, and sexual, as well as neglect on the part of caregivers. Dysfunction within the household, such as drug abuse, mental illness, alcoholism, being witness to violence, and family members being in jail, were also part of the survey. All of these were considered to be adverse experiences for those children exposed to them and were quantified in the survey.
It may also be helpful if I describe what I am calling chronic emotional discomfort. I am including signs or symptoms of either emotional discomfort or distress that appear to become part of the personality structure of the individual with the traumatic experiences. These would include traits like chronic anxiety, long lasting or frequent episodes of depression, chronic insomnia, low self-esteem, and a lack of self-confidence. These types of long-lasting discomfort or dysfunction would also include frequent complaints of physical symptoms when no physical causes can be found to explain them.
Research studies have shown that there is clearly something about early life distress and trauma that is carried forward into later life and disrupts the comfort and peace of mind of those who have endured these experiences. The original ACE study used 8 different categories of adverse experiences and found that they were additive in their impact on later life emotional states. The additive nature of these different kinds of trauma produced a sort of “dose-response” relationship between the total number of different kinds of traumatic experiences and the risk of developing various kinds of chronic emotional discomfort.
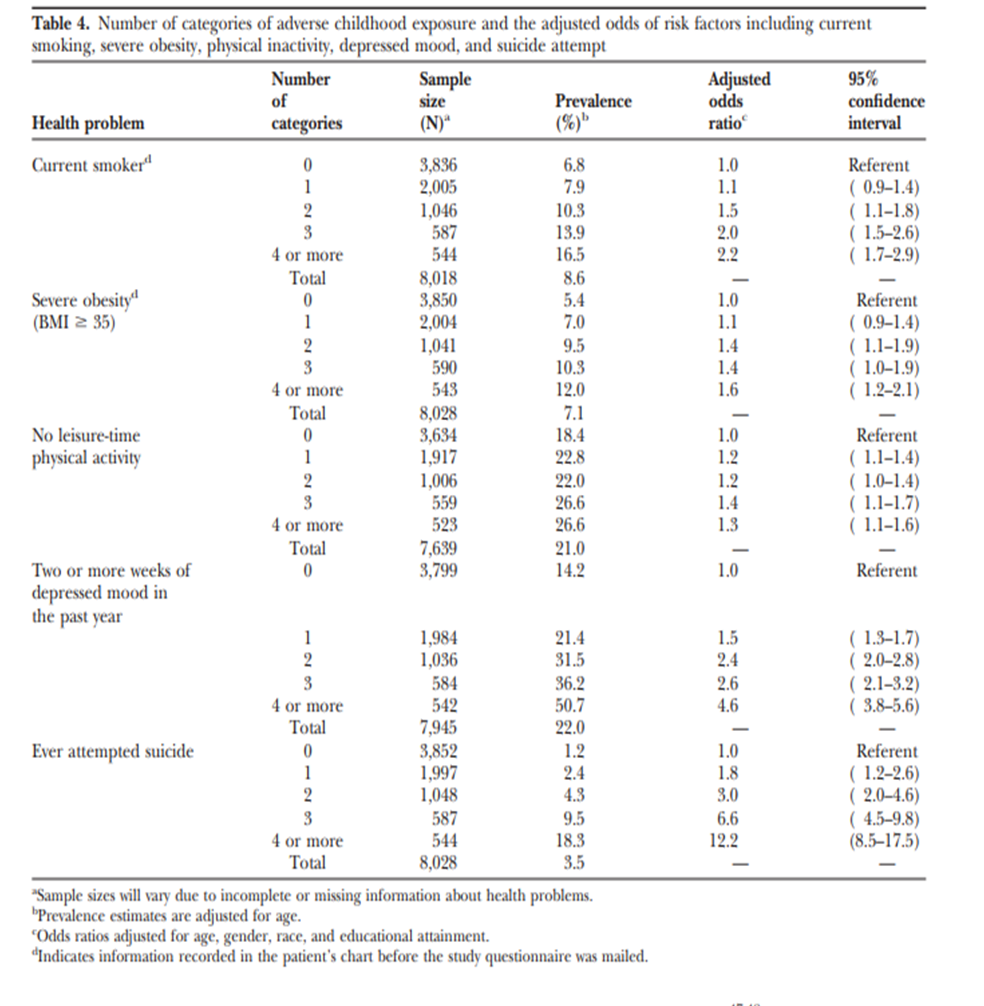
While the total number of early life trauma experiences show the same relationship with all of the different kinds of later emotional symptoms, I will focus here on depression as an example. As the number of ACE’s reported from the survey increased for study subjects, the likelihood of developing depression later in life increased in a graded fashion. For example, for those with no history of abuse or distress reported in the ACE questionnaire, the risk of depression later in life was 14%. For those with 4 or more categories of adverse experience reported, the risk of depression increased to 50.7%. This amounts to a 260% increase in the risk of depression for those with 4 or more ACE’s reported compared to those with none. (See Table 4 in the appendix for more details.) Other research studies have confirmed these findings and have shown that all kinds of chronic discomfort are strongly associated with adverse experiences in childhood.
Since the consequences of early life trauma are found decades later in adult life, they have an enduring, negative impact. Other studies that have specifically examined the effects of early life trauma on adult mental health have found that maturation and time do not reduce the effects. For many of those who have been traumatized, these effects persist across the lifespan. What is it about the experiences of trauma or prolonged emotional distress that is so likely to become embedded in the emotional make-up of the traumatized individual throughout the rest of his or her life? We can look to brain imaging studies of people with a history of ACE’s for a clue. While I will not get into the details at this point, brain imaging studies show specific changes in the structure and function of the traumatized individual’s brain that are clearly associated with these detrimental experiences. (See reference 4 for more details.) Whatever it is that is happening, it tends to become recorded within the neuronal structure of the brain.
I can tell you from what I find in treating people with these emotional problems in my medical practice that standard treatments rarely, if ever, cure the problems. For example, even when anti-depressant medications are effective in completely resolving an episode of depression, more episodes of depression are quite common. In some cases, anti-depressant medications need to be continued long-term, since stopping them results in a rapid return of depression. Another example is the treatment of anxiety. Anti-anxiety medications are usually needed on a chronic basis, and when therapy and counseling are effective, they are also usually needed in the long-term. Low self-esteem, lack of self-confidence and frequent somatic complaints are even less likely to respond to our standard medical or psychological treatments. All of these kinds of emotional problems seem to become permanent personality traits.
Does this mean that there is nothing that can be done to negate the consequences of these experiences? The answer is clearly no, but since we have not been aware of the importance of these factors in the past, this has greatly impeded our ability to develop effective treatments. I will address this vitally important question in detail in a later presentation, but for now I will continue the description of the consequences that are initiated by adverse experiences.
In the next step in my description of an ongoing chain of consequences from adverse experiences, I will describe what the ACE study showed us about how adverse they are often associated with self-destructive habits.
Adverse childhood experiences and detrimental lifestyle choices
How often does the advice of health care workers, friends, and family members result in people stopping the abuse of alcohol, quitting smoking, or avoiding the use of illicit drugs? Clearly, advice is nearly useless and even the threat of going to jail or developing diseases like lung cancer are rarely enough to stop some of these self-damaging habits. Why are they so resistant? The ACE study and similar research reports may be starting to provide answers.
Just like what was found with the risk of emotional problems dramatically increasing with a history of childhood traumas and other detrimental experiences, poor life-style decisions are also strongly associated with these adverse experiences earlier in one’s life. The number of ACE’s reported in the survey were strongly associated with cigarette smoking, alcohol abuse, the use of illicit drugs, obesity, a sedentary lifestyle, and sexual promiscuity. What has been found with all of these detrimental habits is the same kind of dose-response relationship as was found with chronic emotional discomfort. As the number of ACE’s increase, the likelihood of someone acquiring these detrimental habits also increases. (See tables 4 and 5 in the appendix for more details from the original ACE study)
If we select the alcoholism as an example, those with no ACE exposures were found to have a 2.9% risk of being an alcoholic when they were surveyed as an adult. In contrast, for those with 4 or more ACE’s reported, there was a 16.1% risk. This means that someone with 4 or more ACE’s is 455% more likely to become an alcoholic than someone with no ACE’s. Just as we found for the chronic emotional discomfort that was associated with adverse earlier experiences, all the different kinds of detrimental lifestyle choices increased with the total ACE burden.
Are the different kinds of chronic emotional discomfort and the habitual, detrimental habits connected in some way? If you ask people who overeat or who drink alcohol excessively or use drugs, they usually are quite clear in telling you that they feel better while engaging in these self-destructive behaviors. They also report that the even though the benefits are temporary, they still continue their self-destructive behaviors because of the compelling emotional reward they provide. It appears that many poor lifestyle choices are a kind of self-treatment for chronic emotional discomfort. This is probably why they are so difficult to eliminate. In giving advice, we are not addressing the reason the habits develop in the first place, and advice by itself does not help to eliminate the need.
There is yet another important dimension to the problems we are describing here. These are not just individual issues; they are multi-generational. People addicted to drugs or alcohol, those with mental illnesses and those who are chronically angry and abusive as a result of their early life experiences, have children who they then expose to similar distress. If we learn to understand what is going on here and begin to use effective treatments to eliminate the root causes, we will not only be helping our patients, we will also be helping their children and their children’s children.
In the next section of this presentation, I will leave the topics of emotions and behavior and begin to address what the ACE study is telling us that will expand our understanding of the causes of physical disease processes. Physical illnesses are the next step in the chain of consequences that follow adverse experiences.
Adverse childhood experiences and serious physical illnesses
When I first read the results of the original ACE research report, it was the association between childhood trauma and adult physical disease that really surprised me. In the past, when medical scientists considered the risk factors for physical illness, traumatic early life experiences were not something that was considered to be pertinent to explaining why diseases like cancer, heart disease and diabetes develop. A careful review of the research studies that followed the original ACE study report, though, clearly confirms the ACE study findings. We now know that emotional trauma is a potent risk factor for physical illness.
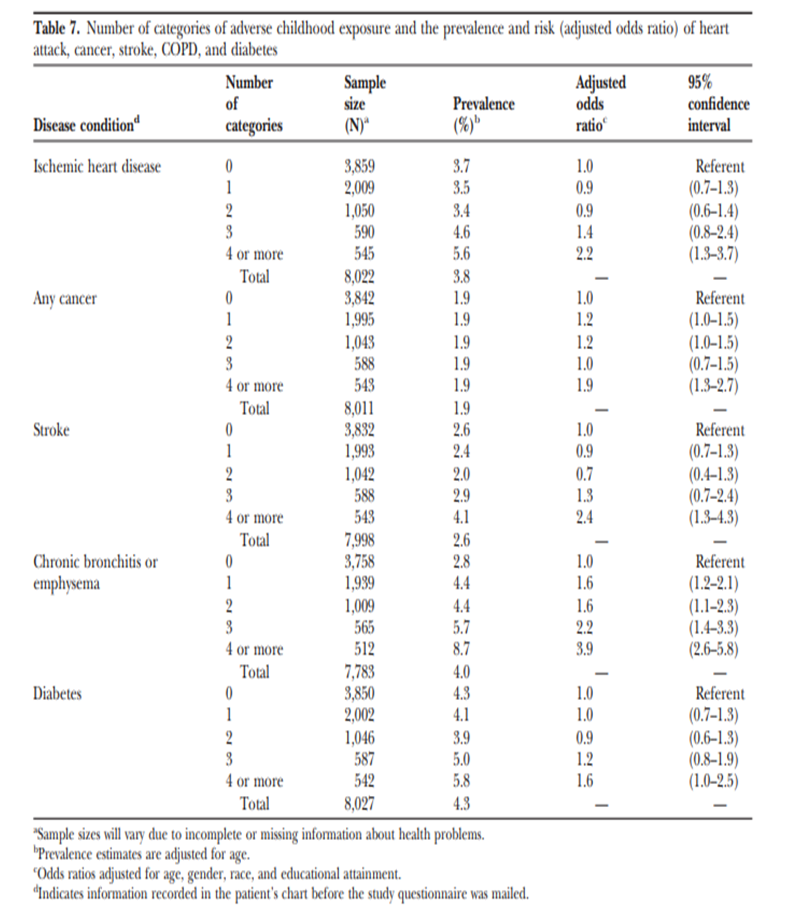
For example, In the original Ace study, 3.7% of adults with no history of childhood trauma were diagnosed with ischemic heart disease. But of the adults with 4 or more categories of trauma in childhood, 5.6% had ischemic heart disease. This means that this disease was much more likely to develop in those who were traumatized as children. If you look at the prevalence of cancer, and you compare those with no trauma history to those with over 4 categories, there is almost twice as many who develop cancer. Diabetes, stroke, COPD, and liver disease also showed a potent dose -response pattern between the number of trauma categories found in the survey and the risk of these diseases. (See table 7 in the appendix for more details)
These results are telling us that emotional trauma in childhood, as measured in the ACE study survey, confers risk that adds to that of the traditional risk factors that medical researchers have focused on in the past. Even when statistical techniques are employed to control for these traditional risk factors, childhood traumas remain as potent factors helping to further explain who will eventually develop these chronic diseases.
Another way to confirm these surprising findings is to look at the lifespan of the people with emotional traumas in their childhood, compare their accumulated trauma burden to their risk of early death. When people from the original study were followed over the next ten years, the lifespan of those with no traumas was 79.1 years. In contrast, those who had reported six or more trauma categories in their childhood, on average, lived only 60.6 years. Incredibly, those with no trauma exposure reported on the ACE survey lived almost 20 years longer than people with a heavy trauma burden from their early life. This is exactly what we would expect if early life traumas are dramatically increasing the likelihood of serious medical illnesses.
Up until this point in this presentation, I have focused primarily on the findings of the original ACE study. It would be a mistake, though, to conclude that the ACE questionnaire captures all of the important traumas and distress that produce chronic illness. Next, I will discuss how these important findings can be expanded to give us an even more accurate understanding of the ways that painful emotional experiences increase the risk that serious physical diseases will develop.
It is not just ACE’s
There are two important ways that we need to expand our understanding of emotional traumas and disease beyond what the ACE study findings have shown us.
First, it is not just childhood. It is clear from the existing research literature that emotional trauma at any point in life has a negative impact on our future emotional and physical health and this impact is clearly additive and cumulative. For instance, studies of soldiers who were surveyed for childhood traumas prior to wartime tours of duty found that those with prior trauma histories were much more likely to develop depression and PTSD after returning to civilian life. Further confirmation is from research studies that have looked at the brain structure changes associated with trauma. They show that the typical changes that follow trauma in childhood also begin to develop following similar traumas later in life.
Second, long-term damage is not limited to the kinds of distress surveyed in the original ACE questionnaire. For example, studies of children who have been bullied show the same kinds of brain changes and the same kinds increased risks of emotional and physical diseases as those found in the original ACE study. Wartime traumas, the loss of loved ones, and being exposed to pervasive social prejudice are also potent risk factors for later emotional and physical illness as well as a higher risk of early death.
We can summarize these research findings by concluding that all kinds of traumatic experience, at any time in life, have these negative consequences. The more intensely distressing and the longer they are continued, the more damage that is done. This is comparatively new information that has not yet changed how the medical profession deals with chronic disease. In the next section, I will endeavor to briefly compare what most physicians and medical scientists still believe about the nature of human disease to what this new data is telling us. We need an updated understanding.
Understanding chronic human disease 2.0
We know that the human body is an amazingly complex organic machine. For several centuries now, we have been accumulating ever greater detail about its structure, metabolic processes, and genetic inheritance. But along with this dramatic increase In our understanding of the mechanics of how the human body operates, we have concluded that its diseases must be the result of, and completely explained by, the physical disruption of the body’s structural components and organs. With this focus on the mechanics, we have lost track of the incredibly important impact of the human mind and emotions on our health. The placebo effect and the “spontaneous remission” of incurable disease, discussed in an earlier presentation, are clear examples of this power of the human mind. In this presentation, the evidence of the chronic damage that emotional trauma creates within our brain and body are further indications of this power.
Along with this modern medical focus on the physical disruptions of the human body as the cause of disease, we have catalogued thousands of named diseases. As we have analyzed these physical determinants of each disease, we have also concluded that each has a unique set of causative factors. In contrast to this modern analysis, in the first presentation of this series, research was presented that demonstrates how religious beliefs and practices tend to heal all disease. While a different set of physical risk factors is associated with each disease process, comforting religious beliefs tend to heal all of these different kinds of diseases in a very general manner. To this understanding we now add that emotional traumas also produce a general tendency in the opposite direction: toward the development of all different kinds of emotional and physical discomfort and disease.
As another consequence of our modern, predominantly physical explanation for why disease develops, there is a large explanatory gap in our ability to predict who will develop chronic disease later in life. The traditionally described physical factors explain less than half of the risk. This large gap in our ability to predict and prevent chronic disease exists because we have not adequately appreciated the true power of the human mind and emotions to either produce damage or promote healing. This has been a major impediment to our efforts to prevent chronic diseases and to slow the aging process
From the results of the research presented here, we have seen that emotionally distressful experiences change the structure of the brain and the metabolic function of the body on a long-term basis. We often experience this damage as anxiety, depression, fatigue, insomnia, and other forms of chronic discomfort or even distress. We have also seen evidence that many of our damaging lifestyle choices are ways to self-manage this chronic emotional discomfort. Eventually, the toxic effects of these emotional states and their metabolic derangements cause the body to breakdown and malfunction, resulting in chronic disease.
I have argued in this discussion that the concept of disease as it was described in the New Testament Gospels points us toward insights that modern science has largely ignored, and that important passages in the Gospels anticipated modern research findings concerning the power of our mind and emotions in promoting either health or disease. To me, it seems clear that what was described in ancient times as “unclean spirits” was the invisible emotional damage and brain structural changes that produce disease. In ancient times, lacking our modern understanding of the human brain and its control of metabolic processes, these effects seemed spiritual and driven by some sort of evil power. The natural conclusion from this ancient model of disease was that the ill person was possessed by this evil power and needed the unclean spirit to be “cast out.” As I have argued earlier, what was being taught by Jesus has the power to heal, even if the ancient understanding of the true cause of disease has resulted in our modern misinterpretation of his true meaning.
This leads to the key question that has motivated me to present this research and the expanded understanding of the causes of human disease that it supports: Can we reverse the damage once it has been acquired, preventing its destructive effects?
Can chronic emotional discomfort and its subsequent physical illnesses be eliminated?
Even though research reports like those based on the ACE questionnaire seem to indicate that adverse experiences and their undesirable consequences usually stay with us for the remainder of our lives, this does not necessarily mean there is nothing we can do about them. One indication is that not everyone who is exposed to childhood trauma suffers the long-term effects. There are circumstances that are somehow protective, even though exactly what they are remains to be better understood. Yet another indication is that being involved with uplifting and inspiring theological teachings leads to long term improvements in our health and well-being. A third indication is that there is now a large research literature that is documenting treatment techniques which help to reverse chronic emotional discomforts such as anxiety, depression, insomnia, and fatigue. While it has not yet been widely accepted and included in modern medical care, treatments that result in long lasting improvement in our emotional state are being shown to also improve our health, prevent disability, and extend our lives.
In the next presentation, I will begin summarizing what we already know about what can be done to better prevent and treat some of the deadliest chronic diseases that often disable us and shorten our lives. You may be surprised by how much has been learned, and by how little it is being put into practice. I will subtitle this presentation: “…and greater works than these shall he do…”
This research promises a lot of benefits both for those we might want to help, and for us, personally, as we work to help others. Psychological benefits include greater peace of mind, increased energy and enthusiasm, increased self-confidence, and better sleep. Physical benefits include lower blood pressure, lower blood sugar, improved immune function, better memory, and prevention or healing of disease in general.
References
This is the original “adverse childhood experiences” research report:
- Felitti VJ, Anda RF, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. Am J Prev Med 1998; 14:245-258
Here are a couple large surveys that confirmed the original ACE report in other populations:
- Bellis MA, Hughes K, et al. Measuring mortality and the burden of adult disease associated with adverse childhood experiences in England: a national survey. J Public Health 2015; 37:445-454
- Llabre MM, Schneiderman N, et al. Childhood trauma and adult risk factors and disease in Hispanics/Latinos in the US: results from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL) Sociocultural Ancillary Study. Psychosom Med 2017; 79:172-180
This research report, published in 2006, includes an excellent survey of what was known about the effect of traumatic experiences on changes in brain structure. In 2006 it was already conclusively demonstrated that traumatic experience is associated with long term detrimental changes in brain structure and function:
- Anda RF, Felitti VJ, et al. The enduring effects of abuse and related adverse experiences in childhood: a convergence of evidence from neurobiology and epidemiology. Eur Arch Psychiatry Clin Neurosci 2006; 256:174-186
This research study used a different survey to measure childhood sources of distress than was used in the ACE study, included a different population, and confirmed the dramatic psychological problems that were found in the ACE study:
- McCauley J, Kern DE, et al. Clinical characteristics of women with a history of childhood abuse: unhealed wounds. JAMA 1997; 277:1362-1368
This research report uses the same database as the original ACE study, but goes into much more detail about the increased risk of ischemic heart disease and mortality form adverse early life experiences:
- Dong M, Wayne GH, et al. Insights into causal pathways for ischemic heart disease: Adverse Childhood Experiences Study. Circulation 2004; 110:1761-1766
The ACE questionnaire covered many of the most common causes of early life trauma but not all. This report adds the damage caused by being bullied as one example of other traumas that impact health and well-being in adults:
- Copeland WE, Wolke D, et al. Adult psychiatric and suicide outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry 2013; 70:419-426
Appendix
The following tables (4, 5 & 7) are from the original ACE study report, cited as reference 1, above:


The human mind is very powerful.